AC Joint Specialist

Are you an athlete who participates in weight lifting, body building or martial arts? If so, you may be at risk of sustaining a shoulder injury to the acromioclavicular joint (AC joint) called osteolysis. Osteolysis of the AC joint is caused by repetitive microtrauma and is marked by an insidious onset of pain in the region of the AC joint. AC joint specialist, Dr. James Mazzara provides diagnosis and both surgical and nonsurgical treatment options for patients in Manchester, South Windsor, Enfield, Glastonbury and surrounding Hartford communities who are suffering from osteolysis of the acromioclavicular joint. Contact Dr. Mazzara’s team today!
What is Osteolysis of the Acromioclavicular Joint?
Osteolysis of the acromioclavicular joint is a process involving the resorption of the distal clavicle. It is usually posttraumatic or may be due to repetitive microtrauma as seen in weight lifting. Pain is localized to the acromioclavicular joint. Radiographs, bone scans or MRIs, in addition to history and physical examination are diagnostic. Plain x-rays alone are usually enough to confirm the diagnosis of osteolysis. Activity modification often helps relieve symptoms but surgery is usually necessary when the symptoms do no improve with conservative treatment.
Disorders of the AC joint are a common cause of shoulder pain and often involve the ligaments, bones, or articular surfaces. Osteolysis of the distal clavicle presents as AC joint pain associated with a loss of subchondral bone detail, AC separation, and cysts adjacent to the articular surface.
Osteolysis has been seen in weight lifters and body builders, those involved in martial arts, and following acute trauma of the AC joint.
Anatomy of the AC Joint
The Ac joint is a diarthrodial joint connecting the convex distal clavicle with the flat of slightly concave acromion. The degree of congruence between these two surfaces is variable. A fibrocartilaginous meniscal disk separates the two articular surfaces in the adolescent. In the adult, the disks are small or poorly defined. The joint is stabilized by the coracoclavicular ligaments (conoid and trapezoid), the AC ligament, and the AC capsule. These ligaments limit the amount of motion allowed at the AC joint to about 10 degrees of rotation as the arm reaches into full elevation.
Etiology of Osteolysis
The mechanical cause of atraumatic osteolysis appears to be repetitive microtrauma to the shoulder. This is frequently seen in weight lifters and athletes. It is now seen more frequently as due to this increased popularity of weight training as a part of fitness programs. Traumatic osteolysis can be seen as a result of a single blunt trauma to the shoulder. The precise cause of the osteolysis is unclear but it is thought to be due to vascular compromise, nervous system dysfunction, microfracture, and stress-induced osteoclastic resorption. The histologic features of microscopic fractures, demineralization, subchondral cysts, and distal clavicle erosion have been described.

Click to Enlarge Image
What are the Symptoms of Osteolysis of the Acromioclavicular Joint?
In both atraumatic and traumatic osteolysis, the patient usually reports a dull ache that is localized over the AC joint. It may radiate to the anterior deltoid or trapezius. With posttraumatic osteolysis, the patient will sometimes relate the onset of pain to a direct blow to the shoulder. Since the traumatic episode may have occurred between 4 weeks to several years prior to the onset of symptoms, specific questions about previous trauma should be asked. These patients may or may not be involved in repetitive physical activity with he affected shoulder.
With atraumatic osteolysis, the patient has an insidious onset of pain in the region of the AC joint. These patients are usually weight lifters or heavy laborers who do not recall a specific injury that may have precipitated their pain. Weight lifters may have more pain while performing bench presses, push-ups, and dips. Patients may note pain at night, with nocturnal awakening when rolling onto the affected shoulder. There may be associated symptoms of popping, catching or grinding. Activities of daily living may become painful as the patient’s symptoms progress.
How do I Know I Have Osteolysis of the Acromioclavicular Joint
Inspection of the affected shoulder may reveal joint prominence or asymmetry. Palpation over the AC joint will reveal tenderness. Provocative tests, such as reaching across to touch the opposite shoulder or placing the hand behind the back, may cause localized pain. Active motion of the shoulder may cause crepitus which must be differentiated from subacromial crepitus.
Motion is rarely restricted, although in long-standing cases mild restrictions of internal rotation and / or cross-body adduction may develop. Restricted motion should be documented by comparing both shoulder. More significant restricted motion in the painful shoulder suggests adhesive capsulitis or glenohumeral arthritis.
The most reliable physical examination test is the cross-body adduction test, in which the arm on the affected side is elevated to 90 degrees and the examiner grabs the elbow and adducts the arm across the body. This will cause pain at the AC joint if there is true pathology in the AC joint. This test may cause pain in posteriorly in patients with subacromial impingement if they have posterior capsular tightness.
In patients with isolated AC joint pathology, an injection of 1ml of 1% lidocaine directly into the AC joint will experience pain relief while patients with subacromial pain or other pathology will still have pain on provocative testing.
Radiographic Evaluation
Standard AP views of the shoulder are usually inadequate to visualize the AC joint. The Zanca view is obtained by angling the x-ray beam 10-15 degrees superiorly and decreasing the voltage to about 50% of that used for a standard glenohumeral exposure.
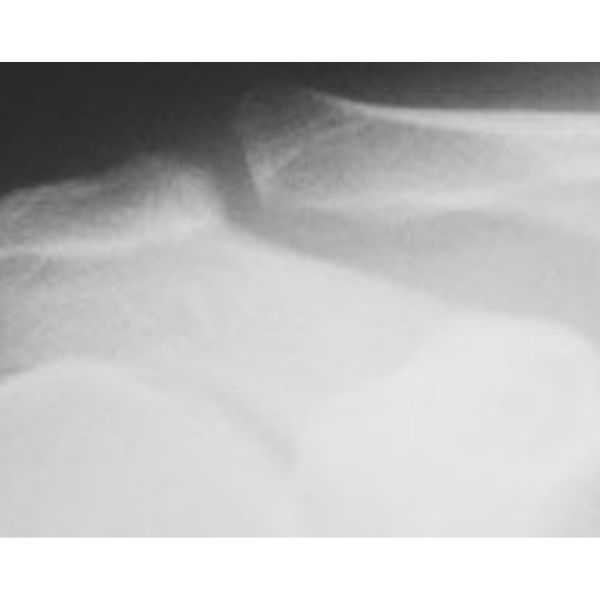
Normal AC joint on Zanca view (Click to Enlarge)
X-rays taken soon after the onset of symptoms may appear normal. Months or years later, the x-rays may reveal loss of subchondral bone detail in the distal clavicle, cystic changes in the subchondral bone, widening of the AC joint, tapering or enlargement of the distal clavicle. The acromion in osteolysis reveals no pathologic changes, differentiating it from AC arthritis.
A bone scan with cone down views of the AC joint will demonstrate increased uptake in the distal clavicle. Scanning is most commonly indicated for the your to middle-aged patient whose symptoms and physical examination are not consistent with plain x-rays.
MRI is rarely indicated for isolated osteolysis. If performed it will show a bright signal in the distal clavicle on T-2 weighted images, signifying edema. Atraumatic and traumatic osteolysis will have similar MRI findings.
Joint Injection for Osteolysis of the Acromioclavicular Joint
Diagnostic uncertainty can be resolved through direct injection of local anesthetic into the AC joint. Elimination of pain within a few minutes of the injection confirms the AC joint as the source of the patients symptoms. This injection test is the most valuable and simplest diagnostic tool.
Relief after the injection is also a good prognostic indicator of the success with distal clavicle resection. Persistence of pain after AC joint injection suggests an additional of a completely different diagnosis depending on the degree of pain relief. The most common alternative diagnosis includes rotator cuff impingement. A second injection into the subacromial space may help clarify the degree to which the patients symptoms are due to impingement as opposed to osteolysis.
Injections into the AC joint can be difficult due to the variable obliquity of the joint surface, sometimes combined with osteophytes and joint narrowing. Reviewing the x-rays and experience in such joint injections are important in successful joint injections.
| Rotator cuff impingement | Differentiate via physical exam, injection test, X-rays |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
What are the Treatment Options for Osteolysis of the Acromioclavicular Joint?
Treatment options must be individualized to the patient. Factors to be considered include the patients age, activity level, shoulder dominance, occupation, degree of activity restriction and / or athletic limitation, and goals.
Do I Need Surgery for Osteolysis of the Acromioclavicular Joint?
Initial treatment should be nonoperative and includes activity modification, ice or moist heat (whichever the patient prefers), nonsteroidal anti-inflammatory medications, corticosteroid injections.
Weight lifters should avoid bench presses, dips, flies, push-ups and any other lifts that elicit pain.
Steroid injections provide short-term relief but do not appear to have any long-term benefits. If administered, patients should avoid provocative activity for one week after the injection. General recommendations include no more than 3 corticosteroid injections in a 3 – 6 month period.
Physical therapy is generally not effective unless patients also have some other concurrent shoulder pathology.
What is Osteolysis of the Acromioclavicular Joint Surgery?
Patient’s who do not respond to nonoperative treatment or who cannot limit their activities may benefit from surgery.
Open and arthroscopic distal clavicle resection have been successful in relieving pain and allowing patients to return to their prior activity level. Open distal clavicle resection, is simple but requires a 4-5 cm incision. It also requires the partial detachment of the deltoid muscle and therefore patients must avoid strenuous for 4 weeks following the surgery.
An arthroscopic distal clavicle resection may be more a difficult procedure to perform but its limited deltoid release allows patients to resume activity when comfortable and requires 3 small 1/4 inch incisions that heal with a more cosmetically acceptable result. Approximately 15 millimeters of distal clavicle is resected.
In our practice, all distal clavicle resections are performed arthroscopically for osteolysis.
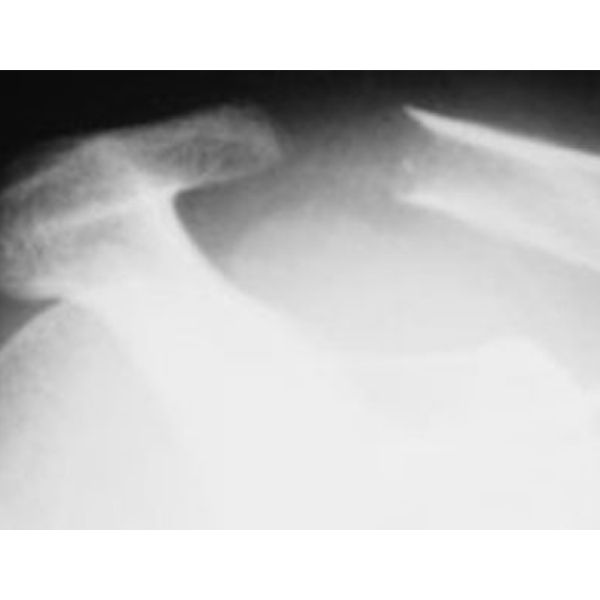
Post operative x-ray demonstrating distal clavicle resection (Click to Enlarge)
Following the surgery, patents are encouraged to use the arm as tolerated. Home exercises are initiated within 1 – 2 days after surgery and physical therapy is started after the first post-operative visit.
Overhead activities are discouraged for 2 – 3 weeks. Most patients will be able to return to full activity at 2 – 3 months after surgery. Patients who also have concomitant tendon problems and require additional work for that problem may require longer to return to normal activities.
Outcomes after arthroscopic distal clavicle resection have generally been excellent. Most studies have reported good to excellent results in the range of 83% to 100%. Our own results have been at the upper end of this range.
Inadequate pain relief following an arthroscopic distal clavicle resection for osteolysis may be due to diagnostic inaccuracy, inadequate distal clavicle resection, AC joint instability or shoulder weakness due to subtle instability of the AC joint.
Summary of Osteolysis of the Acromioclavicular Joint
The patient with osteolysis of the distal clavicle usually reports a dull ache over the superior aspect of the shoulder which is aggravated by specific physical activities. History, physical examination and plain x-rays are usually sufficient to confirm the diagnosis. Initial treatment involves activity modification, NSAIDs and corticosteroid injections for temporary relief. If nonoperative treatment fails and patients are not willing to modify their activities or live with the pain, operative resection of the distal clavicle often provides good to excellent results with few complications.
References
- Shaffer, BS: Painful Conditions of the Acromioclavicular Joint, JAAOS, 7(3), 176-188, 1999.
- Stephens, M; Wolin, PM; Tarbet, JA; Alkayarin, M: Osteolysis of the Distal Clavicle. The Physician and Sports Medicine. 28(12), 2000.