After almost 20 years in practice, I tend to see a lot of interesting patients and x-rays. Below are some x-rays from patients who have come to me from “another surgeon”.
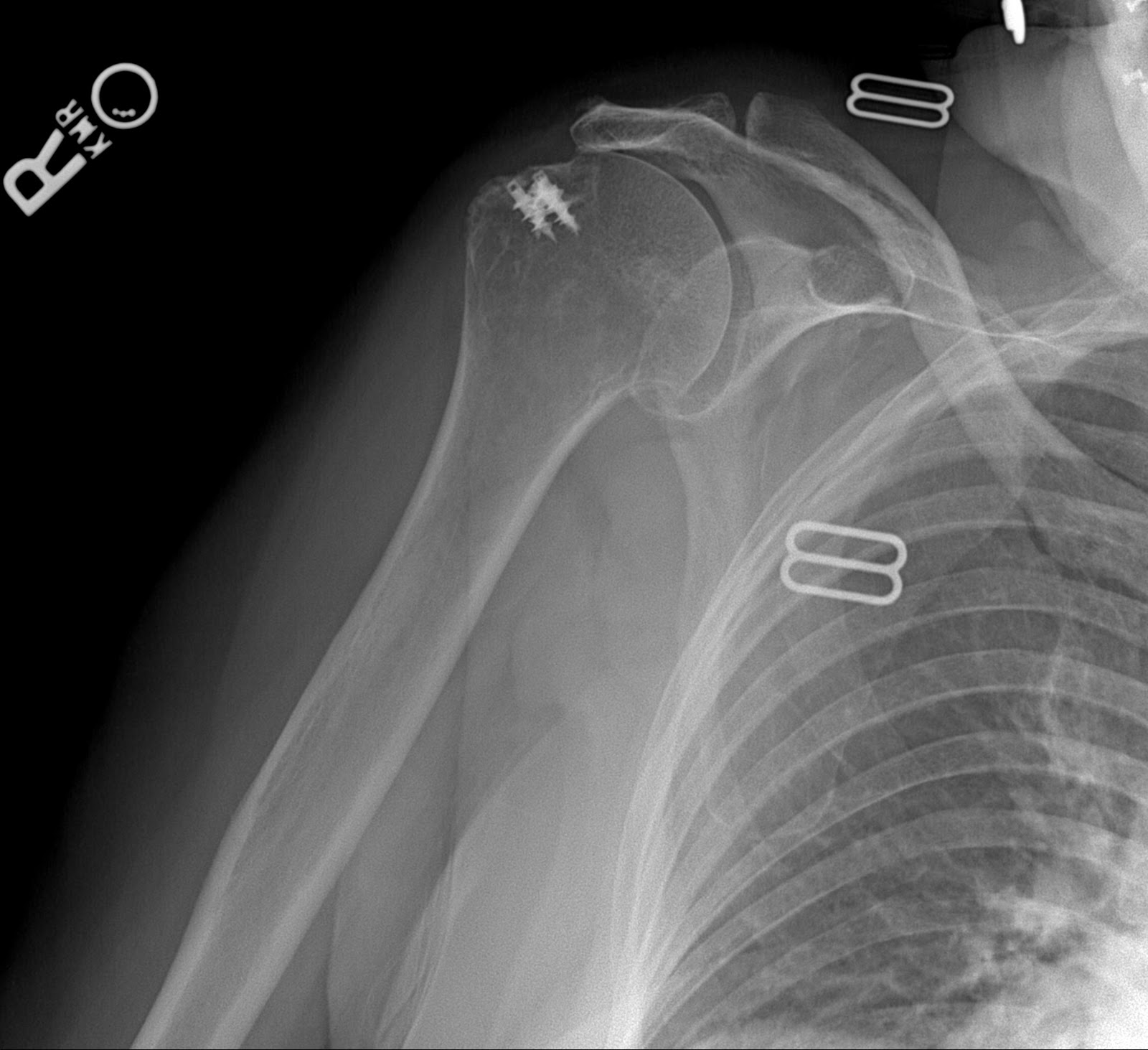
Each patient has had an arthroscopic rotator cuff repair by another surgeon. The first set of films demonstrate that the metal anchors have pulled out of the very soft bone and as a result the tendon has retorn after a rotator cuff repair. This failure was within the first year. This patient was in therapy for many months and could never lift her arm after the repair. Her pain was considerable and she became very unhappy with the situation and eventually came to me for help. A simple x-rays tells the whole story. No MRI needed here. The only set of post operative x-rays done were those done in my office about a year after surgery.
The fact that the anchors are now out of the bone, floating in the joint, indicate that this mechanism of failure. Rotator cuff tendon quality also affects the success of a tendon repair. Poor quality tendon in more likely to retear. Larger tears involving more than one of the 4 rotator cuff tendons will have a higher failure rate as well. Patients over 65 years of age and chronic tendon tears will also have higher rates of failure.
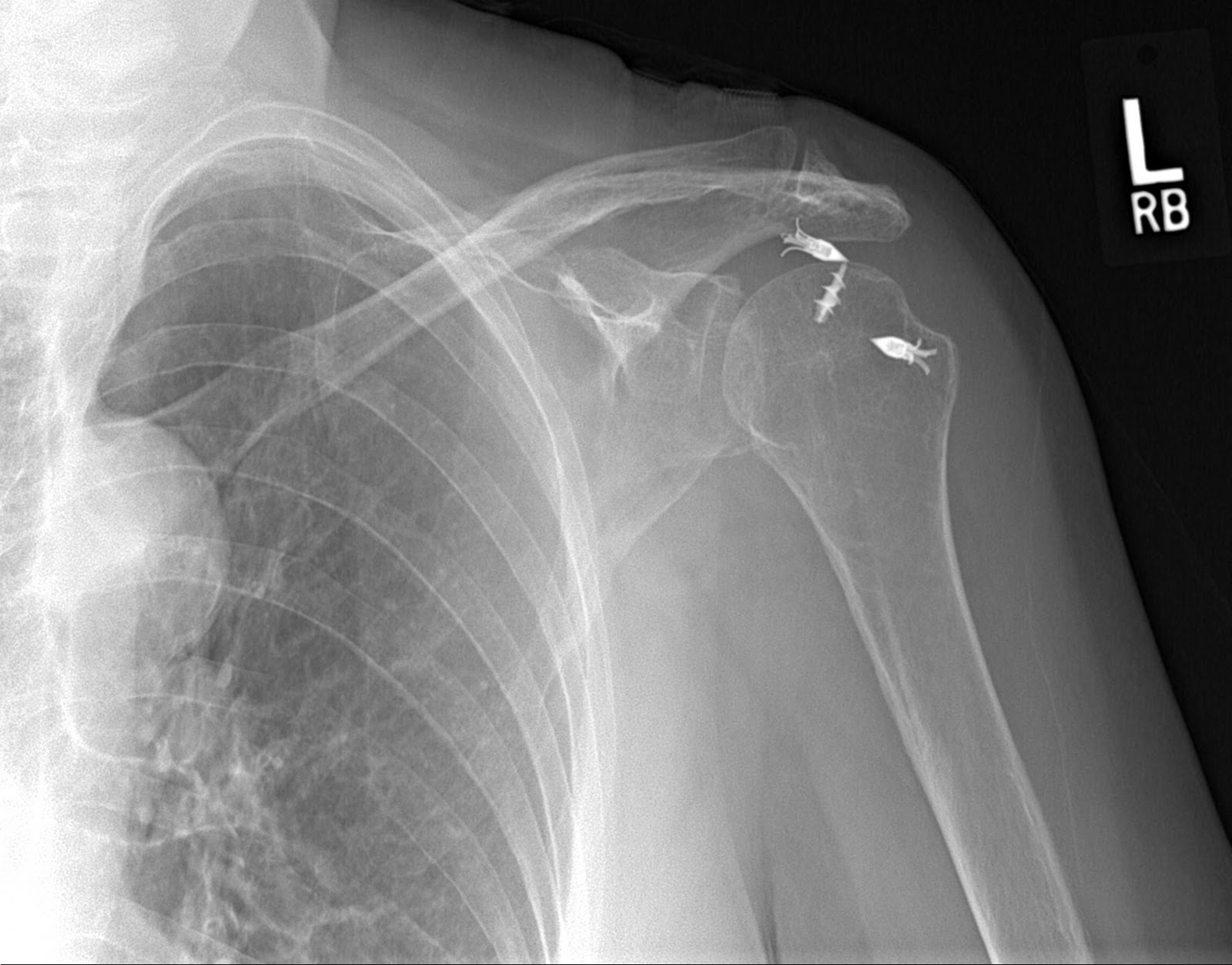
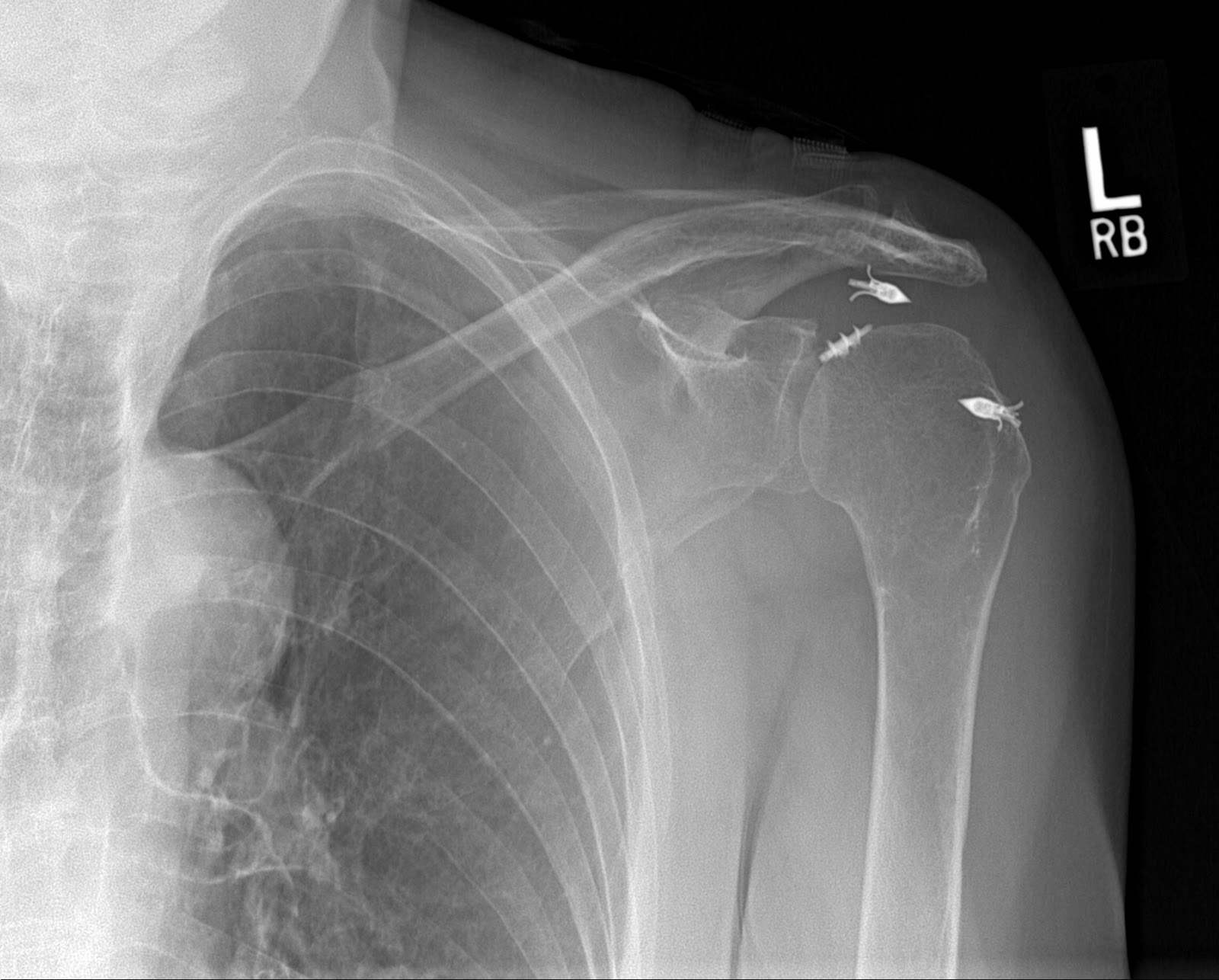

Notice the metal anchors above that seem to be floating in the joint. This foreign body in the joint is very painful. I did surgery on the above patient to remove the anchors arthroscopically. Her pain improved, but her function never recovered. Although I thought she would have done well with a reverse total shoulder replacement, she said that she had enough surgery. I advised her about the limits of surgery under these conditions and, after surgery, she was happy that her pain was improved.
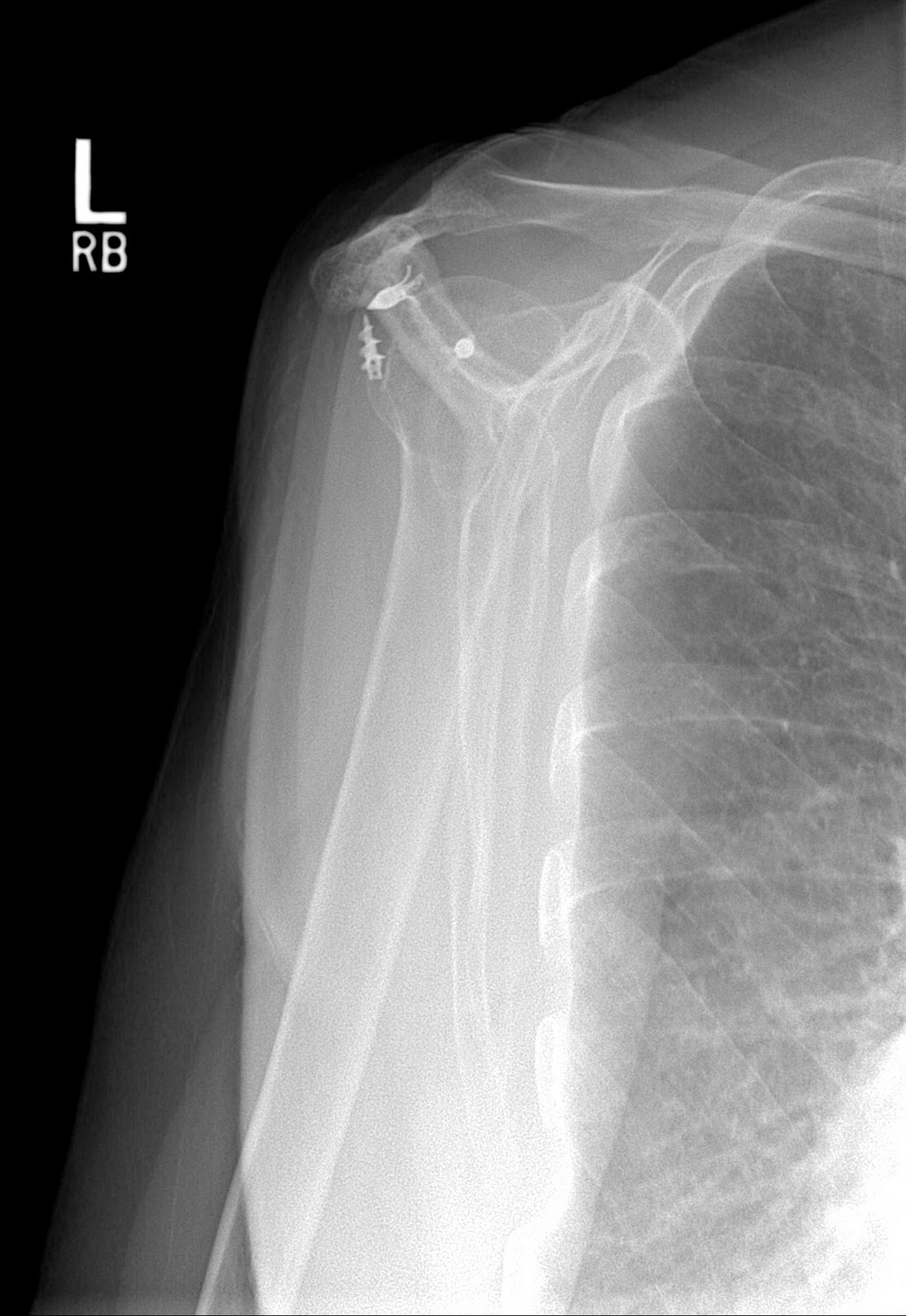
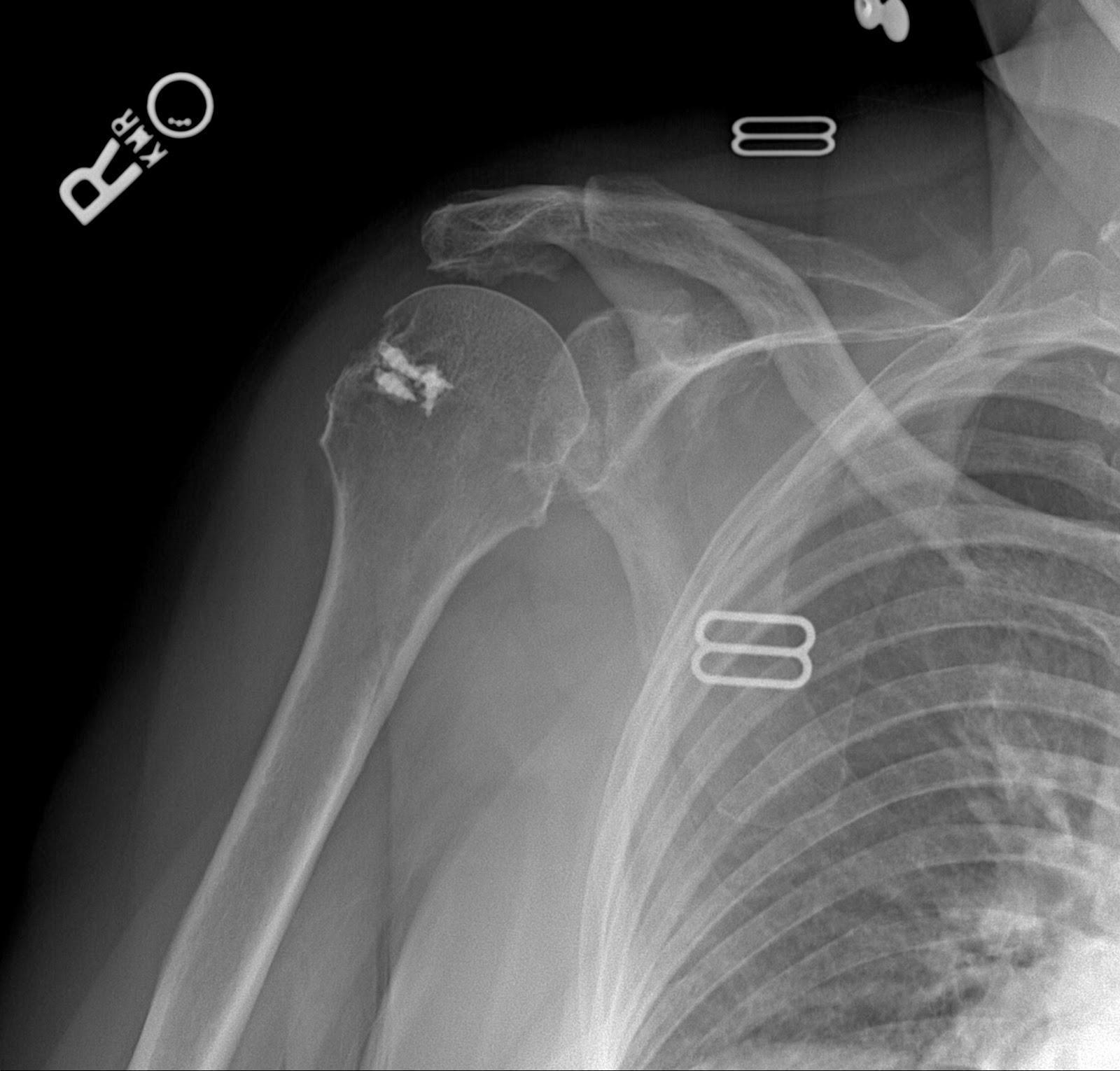
The x-rays below are from a different patient but the operation was by the same surgeon. In this patient, there is moderate pain because the anchors remain in the bone. The repair has failed. If you look carefully, you can see that the head of the humerus (the bone with the metal anchors) has moved upwards and now is touching the bone above it (the acromion). This can only happen when there is a massive rotator cuff tear. Once again, no MRI needed. This patient cannot lift her arm at all and has what we call a pseudoparalyitc shoulder.
{kind=link}
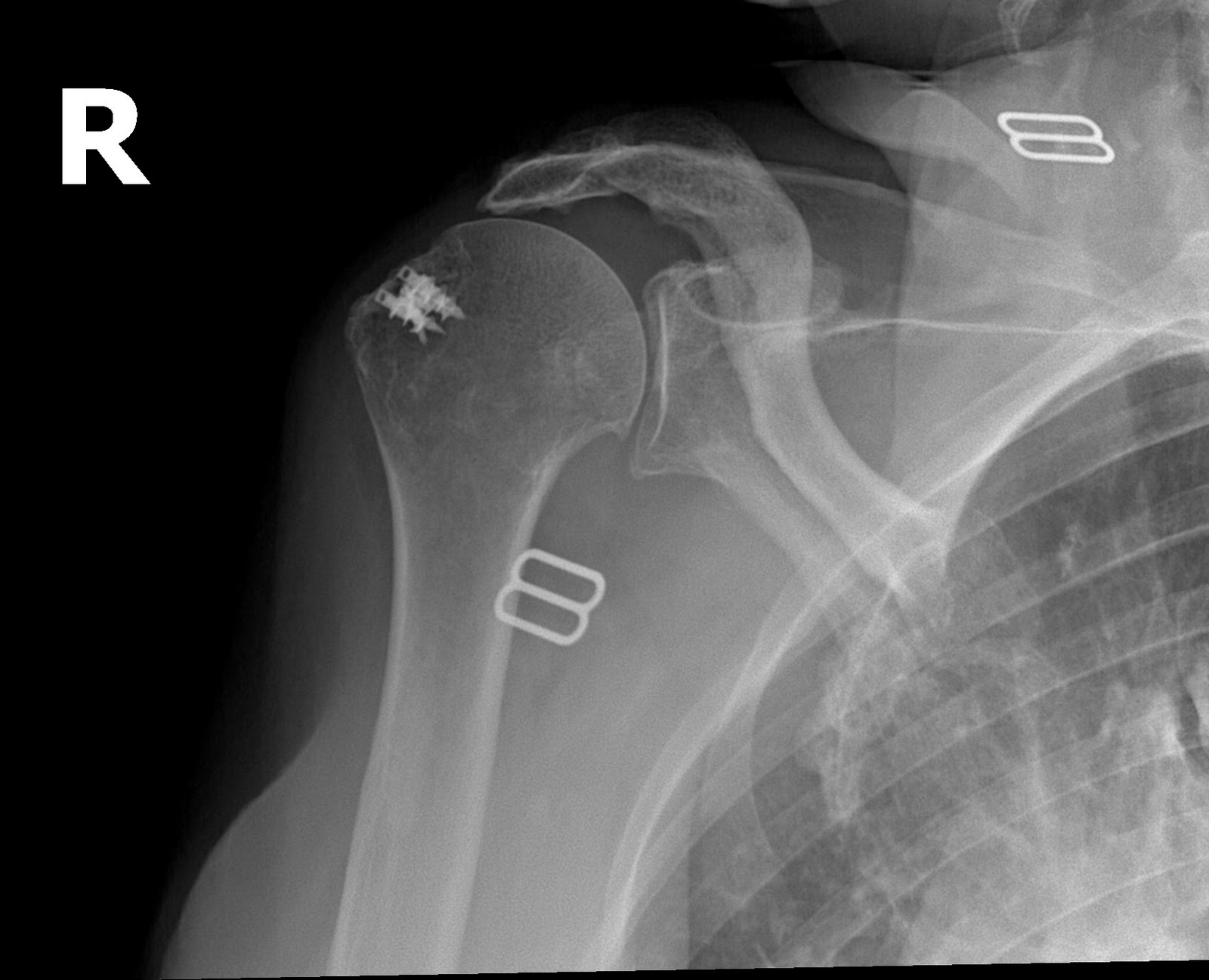

This patient is considering a reverse should arthroplasy. She is the same age as the first patient but much more active. I suspect she would do well with the new shoulder.
Every surgeon who does rotator cuff surgery will have some failures of their repairs. It is just the nature of this type of surgery. Sometime we know at the time of surgery that the repair is tenuous and is at risk for retearing. These patients came to me because their surgeon did not pay much attention to them when they said they were in pain and could not lift their arm. The lesson here is that you should listen to your patient. Pain is normal in the recovery period after any surgery, but if a longer than usual period of time has passed, and the patient cannot lift their arm or has pain, there is usually a reason. It is our job as orthopedic surgeons to try to get that answer. The problem may not always be fixable and the answer may not always be what the patient wants to hear, but we should try to find the answer and recommend a treatment if appropriate.
Here is a excerpt from an article in the Journal of Bone and Joint Surgery, 2001.
Revision Rotator Cuff Repair: Factors Influencing Results by M. DJURASOVIC, MD, et. al.
The causes of clinical failure of rotator cuff repair in any particular case are often multifactorial, but failure of tendon-healing is frequently a factor. The most common causes of failure of tendon-healing include the size of the tear (which is determined by both its anterior-posterior dimension and the degree of retraction), the quality of the tissue, the chronicity of the tear, and the degree of muscle atrophy. These specific factors may be interrelated as they often occur concomitantly in many patients with failed primary rotator cuff repairs. Surgically related reasons for the clinical failure of primary rotator cuff repair include inadequate subacromial decompression, severe subacromial scarring, and untreated symptomatic acromioclavicular arthritis.
Thanks,
JTM, MD