Here is a great review of steroid injections for the painful shoulder. It is very technical and probably better for the medical professional rather than the average patient.
JTM, MD
From International Journal of Clinical Practice by Allen D Bell, MD ; Doug Conaway, MD
Summary and Introduction
Summary
The painful shoulder is a common clinical entity with a broad array of possible causes. A caregiver for an affected patient needs to determine the etiology for the pain, often relying primarily on the history and physical examination and supplemented with laboratory testing and imaging when needed. However, initial treatment decisions are often made before ordering these tests in situations not involving trauma. Most conditions affecting the shoulder are treated with conservative measures such as rest, physical therapy and analgesics.
When such measures fail, local corticosteroid injections can be a valuable tool to help achieve symptom relief for a wide range of the most common conditions affecting the shoulder joint. This review aims to help the clinician distinguish among the commonly encountered causes of shoulder pain and guide therapy when the use of local corticosteroid injections is considered.
Introduction
Historically, injectable corticosteroids, often in combination with physical therapy, have been considered effective and valuable therapy for alleviating joint pain caused by inflammation.[1-4] For over 50 years, clinicians have depended on such local corticosteroid treatment to provide safe, rapid, temporary relief of joint pain and suppression of inflammation.[5-7] Despite this fact, there are few well-controlled studies demonstrating the benefits of injectable corticosteroids for shoulder pain, and hence debate continues regarding which types of shoulder pain are appropriate to treat by injection.[8]
In current practice, corticosteroid injections are among the most accepted, successful and frequently administered treatments employed by rheumatologists, orthopaedic surgeons and primary care physicians.[9] Roughly 90% of orthopedists and 95% of rheumatologists reported using corticosteroid injections for their patients in recent surveys.[10-12] This is likely in part due to the paucity of practical alternatives to surgical intervention.[13]
This review discusses and differentiates the conditions affecting the shoulder, which are candidates for injectable corticosteroid treatment. Corticosteroid injection indications, guidelines, techniques, efficacy and safety are also discussed.
Indications
Injections are appropriate when a symptomatic shoulder condition has a suspected underlying sterile inflammatory component that may respond to corticosteroids. Only commonly encountered conditions are discussed (Table 1). If the cause of an inflamed tendon, bursa or joint is unknown, infection should be excluded before considering the use of corticosteroids.
Table 1. Common Conditions Affecting the Shoulder for Which Corticosteroid Injections May Be of Benefit[17,23,41]
| Osteoarthritis (glenohumeral, acromioclavicular) |
| Rheumatoid arthritis |
| Adhesive capsulitis (frozen shoulder) |
| Rotator cuff impingement/tendinitis/tendinosis |
| Biceps tendinitis |
| Crystal deposition disorders (pseudogout, ‘Milwaukee shoulder’, calcium hydroxyapatite deposition) |
| Subacromial/subdeltoid bursitis |
Rotator Cuff Impingement Syndromes
This broad entity refers to rotator cuff tendinitis/tendinosis and/or partial rotator cuff tendon tears due to impingement. It accounts for the majority of cases of clinically encountered shoulder pain.[14] Such problems are typically encountered in older adults but can be seen in hard-driving young athletes as well. The underlying common pathophysiology is inflammation of the rotator cuff tendons, particularly the supraspinatus tendon, which is the most commonly affected.
Degeneration and/or inflammation of the common tendon of the subscapularis, supraspinatus, infraspinatus and teres minor (i.e. the rotator cuff muscles) most commonly results from overuse, impingement on the tendon from above or below, degenerative changes with aging or microcrystalline deposits.[15]
Impingement of the rotator cuff is common because the tendons must course through a narrow space between the acromion above and the humeral head below (i.e. the impingement interval). This space becomes narrowest when the arm is abducted but is fairly narrow at rest as well; thus, any condition that further decreases this space or enlarges the tendon predisposes to impingement.[15,16] Common possible etiologies include acromial-anatomic variants (e.g. downsloping or curved/hooked acromion, os acromiale), hypertrophic degenerative changes in the acromioclavicular (AC) joints, weight training and a thickened or calcified coracoacromial ligament.[15-17]
Typical patient complaints include limited and/or painful range of motion and weakness, usually of abduction. Pain typically occurs with active range of motion and is worsened with overhead or above-the-shoulder activities, but night pain that disturbs sleep, particularly when the patient lies on the affected shoulder, is another fairly common symptom.[16] Pain is typically located lateral to the glenohumeral joint and is generally less severe at rest.[15] It often radiates laterally to the mid-upper arm.
Examination reveals no restriction of passive range of motion. However, active patient abduction of the affected arm is typically painful along the ‘middle third’ of a 180-degree arc (Figure 1).[15] Decreased strength can also be elicited in this portion of the arc when the physician provides resistance to active motion and can be compared with the opposite side as a point of reference. Other commonly used physical examination maneuvers to demonstrate impingement and the associated rotator cuff tendon irritation include (i) flexing the arm to 90 degrees, then adducting it across the chest; the arm is then internally rotated with force by the examiner, who stabilizes the scapula with his other hand (Hawkins’ test) (Figure 2); and (ii) passively flexing the internally rotated arm into full flexion with the scapula stabilized (Neer’s test) (Figure 3).
 |
Figure 1. (click image to zoom) The arc of elevation maneuver [adapted from (15)]. When a patient with shoulder pain elevates the extended arm from a relaxed, at-the-side position to completely overhead and parallel to the long axis of the trunk, a 180-degree arc is formed. Movement through the first 20-40 degrees (labeled part ‘1’ of the arc) is generally not painful or only minimally symptomatic with rotator cuff tendinitis/tendinosis and impingement, but throughout the portion of the arc designated ‘2’ in the diagram (i.e. the ‘middle third’, approximately 40-120 degrees), pain will occur with active motion. Movement through the terminal 30-60 degrees (labeled ‘3’) of the arc is generally much less painful with rotator cuff pathology and typically affected by acromioclavicular arthritis/ pathology. The exception is when acromioclavicular arthritis and hypertrophic degenerative change are the cause of rotator cuff impingement, in which case both the second and the third labeled portions of the arc will be painful. Patients with glenohumeral arthritis, adhesive capsulitis, acute calcific tendinitis and subacromial bursitis often have pain throughout all the portions of the arc. |
 |
Figure 2. (click image to zoom) Hawkins’ test for rotator cuff impingement. The arm is flexed to 90 degrees, adducted across the chest, then internally rotated forcefully by the examiner, who stabilizes the scapula with his other hand. |
 |
Figure 3. (click image to zoom) Neer’s test for rotator cuff impingement. The arm is internally rotated, then passively lifted into full flexion with the scapula stabilized. |
The ‘drop arm’ test will detect complete rotator cuff tears, the potential end result of continued impingement on degenerating and/or partially torn rotator cuff tendons: gentle downward pressure exerted by the physician on the forearm of an extended arm abducted to 90 degrees cannot be resisted and the arm drops or rapidly falls back to the patient’s side.[14] Another easy test is to simply ask the patient to actively abduct the arm from its resting position at the side – a patient with a full-thickness rotator cuff tear will be unable to do so. Magnetic resonance imaging (MRI), contrast arthrography or ultrasound is often used to confirm the diagnosis of a full-thickness tear if surgical intervention is being contemplated.[18]
Subacromial/Subdeltoid Bursitis
The subdeltoid bursa lies in the subacromial space over the rotator cuff tendons, providing them with lubrication and protection against friction.[16] This bursa does not normally communicate with the glenohumeral joint space, though it can do so in the presence of a full-thickness rotator cuff tear.[13]
Subacromial/subdeltoid bursitis is usually secondary to surrounding irritation (e.g. partial rotator cuff tears, AC joint hypertrophy) or can be primary in rheumatoid or other inflammatory arthritides. A typical history is that of acute severe pain superimposed on a history of chronic milder pain. Tenderness may be elicited along the acromial border laterally, and there is often pain throughout the 180-degree arc of active motion (Figure 1).[17,19]
Calcific Tendinitis
Calcific tendinitis is inflammation/irritation caused by calcium hydroxyapatite deposits around the shoulder, most commonly in the supraspinatus tendon. The exact aetiology is uncertain, but many believe initial tendon degeneration predisposes to dystrophic calcium deposition.[15,18] Resorption of the crystals or rupture of the crystals into surrounding bursae can cause acute, severe pain symptoms thought to be related to a chemical irritation. The calcific deposits in the affected tendon(s) are usually visible on plain shoulder radiographs.[18]
A combination of history, physical examination and radiographic findings is needed to make the diagnosis – as symptoms can mimic other causes of shoulder pain, tendon calcifications are often incidental/asymptomatic, and in some cases, radiographs may be negative due to the microscopic size of the calcifications. Most affected patients are middle-aged, and there is a slight female predominance.[18]
Onset of pain is typically rapid. The pain is unrelated to shoulder position or activity and usually does not improve or change with rest, helping to distinguish this condition from impingement syndrome and glenohumeral arthritis. Patients may be unwilling to move the affected arm, and pain is typically out of proportion to objective physical examination findings. Because of the acute and severe nature of symptom onset, corticosteroid injection, non-steroidal anti-inflammatory drugs (NSAIDs) or both are often considered earlier in the treatment algorithm.[17,18]
Glenohumeral Arthritis
The glenohumeral joint is less commonly affected by osteoarthritis than are the knees and hips because it is not a weight-bearing joint.[18] Repetitive overhead lifters (e.g. occupational lifters, weight lifters and athletes) and those with prior trauma are more commonly affected. Chronic rotator cuff tears, neuropathy and other abnormalities affecting the shoulder can also lead to osteoarthritis and degenerative changes of the glenohumeral joint. Patients are typically aged over 50 years and complain of insidious onset of local pain, limitation of motion and/or weakness.[20] The ‘painful arc’ with osteoarthritis is often the full 180 degrees, and crepitus may be present on examination (Figure 1).
In the absence of such risk factors, inflammatory conditions (e.g. rheumatoid arthritis, calcium pyrophosphate deposition disease, calcium hydroxyapatite deposition [‘Milwaukee shoulder’]) or other etiologies (e.g. prior avascular necrosis) should be considered. History, examination and laboratory and imaging tests help differentiate these causes. Osteoarthritis typically results in an insidious onset of chronic pain, and plain radiographs usually reveal joint space narrowing, osteophyte formation, sclerosis and/or subchondral cysts.[4,17,18] Pain occurs with passive range of motion and at rest, helping to distinguish arthritis from rotator cuff impingement syndrome.
Adhesive Capsulitis
This condition describes a global and typically painful decrease in shoulder range of active and passive motion due to adherence of the shoulder capsule to the humeral head. This condition is sometimes referred to as ‘frozen shoulder’.[20][14,15,17] The cause is often long-standing pain that limits shoulder motion; trauma, rotator cuff tears, thyroid disorders and diabetes have been associated with this condition.
AC Joint Arthritis
Radiographic evidence of AC joint arthrosis and hypertrophic degeneration is common in people aged over 40 years but is often incidental and asymptomatic.[18] AC joint disorders may also be traumatic, and hence radiographs may be warranted to exclude fracture or dislocation/separation.[20] In the case of chronic idiopathic or post-traumatic degenerative changes of the AC joint, patients typically present with gradual and insidious onset of superior shoulder pain.
Classically, the pain is aggravated when the patient rolls onto the affected shoulder while sleeping or while the patient reaches across the chest with the affected arm towards the opposite axilla.[20] On physical examination, the hallmarks of diagnosis are tenderness over the AC joint and AC joint pain with passive or active arm adduction across the body.[17,18] Pain can be exacerbated when the examiner has the patient grab the opposite shoulder with the hand of the affected arm and pushes the patient’s elbow towards the ceiling against resistance.[17] Also, the arm can be extended to 90 degrees, then adducted across the chest to elicit AC joint pain (cross-arm test) (Figure 4).
 |
Figure 4. (click image to zoom) Cross-arm test for acromioclavicular joint pain. The arm is extended to 90 degrees, then adducted across the chest. |
Radiographs can help confirm degenerative changes in the AC joint and exclude the uncommon condition known as osteolysis of the distal clavicle, a similarly treated condition that results in resorption of the distal clavicle secondary to prior trauma or repetitive weight training.[17,20] It is important to remember that hypertrophic osteoarthritis of the AC joint is one of the causes of rotator cuff impingement, and patients can therefore present with symptoms and signs of both conditions (Figure 1).
Biceps Tendinitis
The long head of the biceps tendon travels through the bicipital groove between the greater and lesser tuberosities of the humerus and inserts on the superior glenoid/glenolabral complex.[18] Irritation of the long head of the biceps tendon is relatively common and typically occurs due to repetitive shoulder flexion, while the short head of the tendon is less commonly affected clinically.[17] Patients typically complain of anterior shoulder pain and may relate a snapping or popping sensation or sound in the shoulder.
The diagnosis of biceps tendinitis (sometimes called bicipital tendinitis) is based on localising the patient’s maximal site of tenderness to the bicipital groove, where the long head of the tendon lies.[18] Yergason’s supination sign refers to pain in the bicipital groove when patient-initiated forearm supination of a pronated forearm with the elbow at 90 degrees is resisted by the examiner (Yergason test) (Figure 5).[18] A positive Speed’s test refers to pain at the bicipital groove with resisted forward flexion of a supinated forearm while the shoulder is partially flexed.[17]
 |
Figure 5. (click image to zoom) Yergason test for biceps tendinitis. With the elbow flexed at 90 degrees, the patient’s maximised site of tenderness is elicited as the examiner resists the patient’s attempts to supinate his forearm. |
Biceps tendon rupture results in objective weakness of biceps muscle function and often causes ecchymosis at the site of rupture. A bulge in the medial aspect of the distal upper arm (‘Popeye’ muscle) occurs as a result of unopposed contraction of the biceps muscle from the loss of tendon integrity.[16] Most cases are in older patients and are managed conservatively, but the diagnosis can be confirmed with MRI if surgery is being considered.
Selecting Patients for Corticosteroid Injection Therapy
In general, all the above conditions should first be treated with conservative therapies, including rest, physical therapy and analgesics such as NSAIDs. In most cases, such therapy will suffice to alleviate symptoms. Corticosteroid injections are typically reserved for those who fail an adequate treatment regimen using one, or preferably a combination, of the above regimens.[20] The severe and acute nature of symptoms of some of the above-mentioned conditions, such as subacromial bursitis, calcific tendinitis, rheumatoid arthritis, adhesive capsulitis and gout, may warrant earlier treatment with intrabursal or intra-articular corticosteroids to obtain satisfactory pain relief.[1,9,13,15,17,21,22]
In special patient populations, such as those who are intolerant of or at high risk of complications from NSAIDs, corticosteroid injections may be a first-line therapy.[22] Elderly patients and those with gastrointestinal upset or bleeding from NSAIDs, a history of peptic ulcer disease, and renal insufficiency are all at high risk from NSAID therapy. Joint-replacement candidates may also benefit from corticosteroid therapy prior to treatment, since the potential complications of repeated corticosteroid injections are less of a concern.
Injection Techniques
General Guidelines
Selection of Corticosteroid Agent and Dose. Relatively few studies have been published on the pharmacokinetics of intra-articular corticosteroids.[23][24] Though difficult to predict in the individual patient, average duration of action is roughly 1-3 weeks and tends to be longer for the more non-soluble corticosteroid preparations.[21-23,25-27] Less-soluble products may remain in the joint for 2-3 weeks; mean residence time in the joint is roughly 6 days. Selection of a particular injectable corticosteroid is often based on physician’s comfort level and experience (Table 2).
Table 2. Commonly Used Injectable Corticosteroid Preparations [modified from (30)]
| Solubility/generic (trade) name | Dose equivalent, mg* |
|---|---|
| Relatively insoluble | |
| Dexamethasone acetate (Decadron-LA) | 0.75 |
| Hydrocortisone acetate (Hydrocortone) | 20.0 |
| Prednisolone acetate (Prednalone) | 5.0 |
| Triamcinolone acetonide (Kenalog) | 4.0 |
| Triamcinolone hexacetonide (Aristospan) | 4.0 |
| Slightly soluble | |
| Methylprednisolone acetate (Depo-Medrol) | 4.0 |
| Prednisolone tebutate (Hydeltra-TBA) | 5.0 |
| Triamcinolone diacetate (Aristospan Forte) | 4.0 |
| Soluble | |
| Dexamethasone sodium phosphate (Decadron) | 0.75 |
| Prednisolone sodium phosphate (Hydeltrasol) | 5.0 |
| Most soluble | |
| Betamethasone sodium phosphate (Celestone) | 0.6 |
*For example, 4 mg of methylprednisolone acetate is equivalent to 0.75 mg of dexamethasone sodium phosphate, which is equivalent to 5 mg of prednisolone acetate.
A suggested guideline is to use a more water-soluble preparation for acute inflammatory conditions such as tendinitis and a less water-insoluble preparation for chronic inflammatory conditions (e.g. impingement, bursitis and arthritis), recognizing that the trade-off is a shorter duration of action for the more soluble agents.[10,26] Others believe that soluble formulations (e.g. hydrocortisone) have little role in infiltration therapy because they diffuse more readily from the injected region and can exert greater systemic effects.[9] For chronic conditions, preparations of methylprednisolone and triamcinolone are often favored and appear to maximize the anti-inflammatory effects and duration of benefit relative to other currently available corticosteroid formulations.[9,26][28] These were also the most widely used agents among members of the American College of Rheumatology in a previous survey.
The dose to be injected and needle size depend on the specific structure being injected, but are generally the same regardless of the underlying condition affecting each specific site. A proposed guideline for the various injections detailed in this review is provided (Table 3), but prescribing information should always be consulted.
Table 3. Needle Sizes and Doses for Injection of Various Shoulder Structures [modified from (19)]
| Structure | Needle gauge size | Dose of methylprednisolone acetate, mg |
|---|---|---|
| Acromioclavicular joint | 22-25 | 4-10 |
| Biceps tendon (long head) | 22 | 10-20 |
| Glenohumeral joint | 20 | 20-40 |
| Subacromial bursa | 20 | 20-40 |
The objective for any injection procedure is to insert the needle at the selected site in the shoulder with minimal pain and trauma and not introduce infection. For all injections, informed consent should be obtained and patients made as comfortable as possible. Sterile technique should be utilised and gloves worn. The desired entry site should be identified using standard anatomic landmarks and marked (e.g. thumbnail and retracted tip of a ballpoint pen or marker). The skin should be cleaned with betadine, alcohol swabs or chlorhexidine and allowed to dry completely. To minimise patient’s discomfort from the procedure, an ethyl chloride spray may be applied for 5 s, after which a subcutaneous or topical anaesthesia such as lignocaine (lidocaine) can be applied to anaesthetise the shoulder. The operator should allow 3-5 min to ensure that the area is sufficiently anaesthetised before injecting the corticosteroid. The needle is then advanced to the desired point. Prior to injection, the plunger is withdrawn, which may return synovial fluid and confirm the correct location. This also ensures that a blood vessel has not been entered. When a bursa or joint space is injected, the solution should flow easily without significant resistance. An adhesive strip can be used to cover the injection site after the procedure.[29-32]
Specific techniques for injection are somewhat varied but generally uncomplicated and are further delineated below.[4,13] After the procedure, patients should be advised to limit activity for 48-72 h and counseled to use ice and analgesia for rare post-injection ‘flares’ related to chemical irritation from the corticosteroid preparation.[10,25,30,32,33]
Techniques for Specific Sites
Subacromial Injection. Injection into the subacromial/subdeltoid bursal space can be utilized for rotator cuff impingement syndrome, calcific tendinitis, subacromial/subdeltoid bursitis and adhesive capsulitis.[9,17,19] A lateral approach generally is used and is all that is discussed, though other approaches have been described.[13,14,17,19,34]
The affected shoulder is palpated until the distal, lateral and posterior edges of the acromion are identified. The needle is inserted inferior to the posterolateral corner of the acromion, aiming the needle medially and slightly anteriorly under the acromion with the tip directed to the undersurface of the acromion (Figure 6).[9,19] The practitioner may want to gently pull down on the upper arm at the elbow to open up the subacromial space.
 |
Figure 6. (click image to zoom) Subacromial space injection technique to enter the subacromial/subdeltoid bursa [adapted from (9)]. The acromion is the palpable landmark, with the needle entry site and direction illustrated with an arrow in the figure and described in the text. |
Glenohumeral Joint Injection. Injection directly into the glenohumeral joint space can be used for acute and chronic capsulitis (i.e. frozen shoulder), glenohumeral arthritis and synovitis (e.g. rheumatoid arthritis).[9,14,17,19] The posterior entry is preferred by the author owing to the possibility of arterial or brachial plexus injury with an anterior approach, but both anterior and posterior approaches are commonly used.[17,19]
For the posterior approach, the patient’s arm can be internally rotated across the waist, and the needle inserted two fingerbreadths inferior and medial to the posterolateral corner of the acromion and directed antero-medially towards the coracoid process (Figure 7).[9,14,17,19]
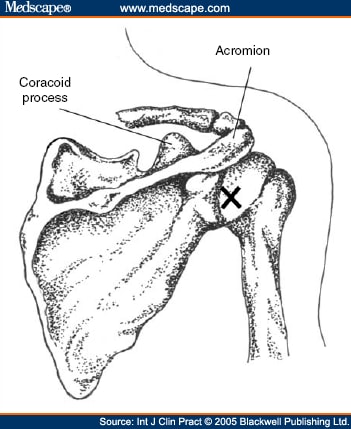 |
Figure 7. (click image to zoom) Posterior approach glenohumeral joint injection technique [adapted from (9)]. The goal of this injection is to enter the glenohumeral joint space. The skin entry site just below and medial to the posterolateral aspect of the labeled acromion is marked with an ‘X’, and from this posterior approach the needle tip is directed towards the labeled coracoid process. |
The anterior approach involves inserting the needle tip a fingerbreadth lateral to and just below the coracoid process and directing the needle posteriorly and slightly laterally.[19,35]
AC Joint. The AC joint space can be palpated about 1 cm medial to the top of the acromion and can be approached for injection from above and from a slight anterior position, though other techniques have been described.[9,17,35] The patient should be seated with the arm hanging down to slightly open the AC joint.[9,17] The needle tip can then be directed inferiorly into the joint (Figure 8).
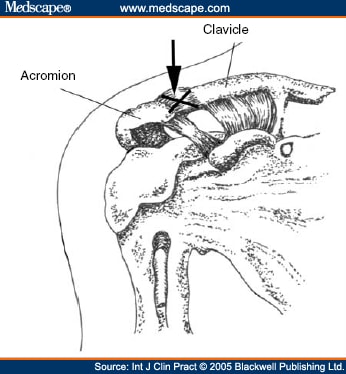 |
Figure 8. (click image to zoom) Acromioclavicular joint injection technique to enter the acromioclavicular joint space [adapted from (9)]. The skin entry site is just above the acromioclavicular joint (which is labelled with an ‘X’) with the needle tip directed inferior as illustrated by the arrow in the figure. |
Biceps Tendon. The goal of this injection is to enter the tendon sheath of the biceps tendon and/or the bicipital groove around the tendon without injecting into the tendon itself.[17,35] The tendon is identified in the bicipital groove of the humerus. A needle is inserted into the skin over the point of maximal tenderness and directed into the groove at an angle with the needle tip nearly parallel to the groove. Increased resistance to flow of the injection should suggest an intra-tendinous location and direct the caregiver to withdraw the needle tip slightly.[17,35]
Efficacy Data
Though anecdotal data are strong, there are somewhat limited controlled trial data to support or refute corticosteroid injections for the painful shoulder.[21,34] An extensive recent meta-analysis by Buchbinder et al.[8] found a benefit of subacromial corticosteroid injection for rotator cuff disease and glenohumeral intra-articular corticosteroid injection for adhesive capsulitis compared with placebo. Short-term benefit has been demonstrated by others (not included in the meta-analysis of Buchbinder et al.) for AC joint pain, adhesive capsulitis and non-specific rest pain of the shoulder.[1,21,36]
The American Academy of Orthopedic Surgeons includes corticosteroid injections as part of its recommended clinical guidelines for the treatment of rotator cuff disorders and AC joint pain, and the American College of Rheumatology has advocated corticosteroid injections to primary care providers for glenohumeral synovitis (e.g. rheumatoid arthritis), adhesive capsulitis (frozen shoulder), rotator cuff tendinitis, impingement syndrome, subacromial bursitis and AC joint arthritis.[9,20]
Contraindications and Complications
Contraindications. Contraindications to intra-articular corticosteroid injection include infection in or around the joint (e.g. septic arthritis, periarticular cellulitis and osteomyelitis), bacteremia or sepsis, significant skin breakdown at the proposed injection site, known hypersensitivity to the proposed injection, the presence of a joint prosthesis, uncontrolled bleeding diathesis, osteochondral or other intra-articular fracture and severe joint destruction (e.g. Charcot’s joint).[26,28,30,31]
Relative contraindications include joint instability, adjacent superficial skin lesions or abrasions, hemarthrosis, severe osteoporosis of bones adjacent to the joint and an uncooperative patient.[26,28,30,31] Diabetic patients should be warned that corticosteroid injections can cause elevation of their blood sugar for 2-3 days after the procedure. Caution should also be used in patients on anticoagulation therapy. Equally important is for the practitioner to make sure that one is not using injectable corticosteroids for a condition that would not be expected to be helped by the treatment (e.g. acute injury, pathology due to neurogenic disease, referred pain and neuropathic arthritis).
Complications. The administration of intra-articular corticosteroids is generally safe with minimal risk to the patient when used conservatively, appropriately, and with aseptic technique.[37] As with any pharmacological agent, corticosteroids should not be administered indiscriminately, however, and no treatment is without risk.
Reported side effects of corticosteroid injection therapy include systemic effects, tendon weakening/rupture, fat atrophy, muscle wasting, skin pigment changes, septic arthritis, nerve and blood vessel damage, post-injection symptom flare/synovitis, facial flushing, anaphylaxis and steroid arthropathy.[10,22,30,32] Almost all these complications can be minimized or prevented by taking a careful history, using an accurate and aseptic injection technique, and avoiding high doses and overly frequent injections.[10,22,30,32] Most clinicians recommend at least a 3-month interval between corticosteroid injections to help prevent certain steroid-related complications, though little scientific data support this specific interval.[26,28,30]
The most common significant clinically encountered side effect is likely the steroid flare reaction, which occurs in up to 5% of intra-articular injections. Flares probably are caused by inflammation related to phagocytosis of the corticosteroid crystals by leucocytes.[9,32] The pain from this side effect typically starts a few hours after the injection and stops within 24-48 h as the anti-inflammatory effect of the glucocorticoid overrides the inflammatory effect of the corticosteroid crystals.[9,32] Treatment includes rest, cold compresses and analgesics.[9,32,33]
Injections directly into a tendon can cause rupture; this is particularly important to remember when performing subacromial and biceps tendinitis injections.[4,38,39] Several case reports of avascular necrosis in months following corticosteroid injection have been published, but no causal evidence exists.[23][4] The feared complication of introducing infection into a joint has an exceedingly low incidence if standard aseptic technique is used, and has been estimated in the range from 1 in 15,000 to 1 in 85,000 in larger series.[30,40] There is a much stronger association for avascular necrosis with prolonged use of systemic corticosteroids, and the shoulder seems to be affected more than other upper limb joints.
Conclusion
Shoulder pain is a common clinical complaint, and a combination of history, physical examination, laboratory testing and imaging may be needed to determine the underlying cause of pain. Once the diagnosis is established, conservative measures are generally employed and give most patients symptomatic relief.
When initial conservative therapy fails, or for patients who have severe, acute symptoms, depot corticosteroid injections are a well-established therapy for painful shoulder joints and have a long track record of safety. Proper technique and accurate pre-procedural diagnosis help to assure the maximum benefit and safety of this treatment.
References
- Carette S, Moffet H, Tardif J et al. Intraarticular corticosteroids, supervised physiotherapy, or a combination of the two in the treatment of adhesive capsulitis of the shoulder: a placebo-controlled trial. Arthritis Rheum 2003; 48: 829-38.
- Rasmussen S, Lorentzen JS, Larsen AS, Thomsen ST, Kehlet H. Combined intra-articular glucocorticoid, bupivacaine and morphine reduces pain and convalescence after diagnostic knee arthroscopy. Acta Orthop Scand 2002; 73: 175-8.
- Jones A, Doherty M. Intra-articular corticosteroids are effective in osteoarthritis but there are no clinical predictors of response. Ann Rheum Dis 1996; 55: 829-32.
- O’Driscoll SW. Surgery of the shoulder arthritis. In: Koopman WJ, ed. Arthritis and Allied Conditions: A Text of Rheumatology, 13th edn. Baltimore, MD: Williams & Wilkins, 1997: 899-911.
- Lane NE, Thompson JM. Management of osteoarthritis in the primary-care setting: an evidence-based approach to treatment. Am J Med 1997; 103: S25-30.
- Uthman I, Raynauld JP, Haraoui B. Intra-articular therapy in osteoarthritis. Postgrad Med J 2003; 79: 449-53.
- Hollander JL, Brown EM Jr, Jessar R, Brown C. Hydrocortisone and cortisone injected into arthritic joints; comparative effects of and use of hydrocortisone as a local antiarthritic agent. J Am Med Assoc 1951 2004; 147: 1629-35.
- Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain (Cochrane Review). In: Anonymous. The Cochrane Library, Issue 1, Chichester, UK: John Wiley & Sons Ltd, 2004.
- Canoso JJ. Corticosteroid infiltrations (Available at http://www.rheumatology.org/publications/primarycare/number5/hrh0029598.asp, accessed June 9 2004).
- Fadale PD, Wiggins ME. Corticosteroid injections: their use and abuse. J Am Acad Orthop Surg 1994; 2: 133-40.
- Hochberg MC, Perlmutter DL, Hudson JI, Altman RD. Preferences in the management of osteoarthritis of the hip and knee: results of a survey of community-based rheumatologists in the United States. Arthritis Care Res 1996; 9: 170-6.
- Hill JJ Jr, Trapp R, Colliver J. Survey on the use of corticosteroid injections by orthopaedists. Contemp Orthop 1989; 18: 39-45.
- Bamji A. The painful shoulder. Practitioner 2001; 245: 1005-17.
- Kalb RL. Evaluation and treatment of shoulder pain. Hosp Pract (Off Ed) 1998; 33: 119-22.
- Canoso J. Regional pain syndromes: diagnosis and management, 2004 (Available at. http://www.rheumatology.org/publications/primarycare/number5/hrh0026598.asp?aud=mem, accessed January 13 2005).
- Fongemie A, Buss D, Rolnick SJ. Management of shoulder impingement syndrome and rotator cuff tears. Am Fam Physician 1998; 57: 667-82.
- Tallia AF, Cardone DA. Diagnostic and therapeutic injection of the shoulder region. Am Fam Physician 2003; 67: 1271-8.
- Martin SD, Thornbill TS. Shoulder pain. In: Ruddy S, Harris ED Jr, Sledge C, eds. Kelley’s Textbook of Rheumatology, 6th edn. Philadelphia, PA: Saunders, 2001: 475-508.
- Pfenninger JL. Injections of joints and soft tissue: part II. Guidelines for specific joints. Am Fam Physician 1991; 44: 1690-701.
- American Academy of Orthopedic Surgeons. AAOS clinical guideline on shoulder pain support document, 2001 (Available at http://www.aaos.org/wordjtml/pdfs_r/guideline/suprt_08.pdf, accessed June 9, 2004).
- Roy S, Oldham R. Management of painful shoulder. Lancet 1976; 1: 1322-4.
- Owen DS Jr. Aspiration and injection of joints and soft tissues. In: Ruddy S, Harris ED Jr, Sledge CB, eds. Kelley’s Textbook of Rheumatology, 6th edn. Philadelphia, PA: Saunders, 2001: 583-603.
- Caldwell JR. Intra-articular corticosteroids. Guide to selection and indications for use. Drugs 1996; 52: 507-14.
- Derendorf H, Mollmann H, Gruner A, Haack D, Gyselby G. Pharmacokinetics and pharmacodynamics of glucocorticoid suspensions after intra-articular administration. Clin Pharmacol Ther 1986; 39: 313-7.
- Schumacher HR Jr. Aspiration and injection therapies for joints. Arthritis Rheum 2003; 49: 413-20.
- Hunter JA, Blyth TH. A risk-benefit assessment of intra-articular corticosteroids in rheumatic disorders. Drug Saf 1999; 21: 353-65.
- Hollander JL. The use of intra-articular hydrocortisone, its analogs, and its higher esters in arthritis. Ann N Y Acad Sci 1955; 61: 511-6.
- Rozental TD, Sculco TP. Intra-articular corticosteroids: an updated overview. Am J Orthop 2000; 29: 18-23.
- Schumacher HR Jr. Arthrocentesis of the knee. Hosp Med 1997: July: 60-64.
- Lanyon P, Doherty M. Intra-articular therapy. In: Firestein GS, Panayi GS, Wollheim FA, eds. Rheumatoid Arthritis: Frontiers in Pathogenesis and Treatment Oxford: Oxford University Press, 2000: 361-9.
- Cellular Aspects of Rheumatoid Arthritis. Intrasynovial Injection Techniques Kalamazoo, MI: The Upjohn Company, 1982: 1-29[booklet].
- Noerdlinger MA, Fadale PD. The role of injectable corticosteroids in orthopedics. Orthopedics 2001; 24: 400-5.
- American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: rheumatologists in the United States. Arthritis Rheum 2000; 43: 1905-15.
- Naredo E, Cabero F, Beneyto P et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol 2004; 31: 308-14.
- A How to Reference Guide. Periarticular and Intra-Articular Injections Kalamazoo, MI: Pharmacia, 2002.
- Jacob AK, Sallay PI. Therapeutic efficacy of corticosteroid injections in the acromioclavicular joint. Biomed Sci Instrum 1997; 34: 380-5.
- Hollander JL. Intrasynovial steroids for rheumatoid arthritis. Med Counterpoint 1974; 37-8.
- Karpman RR, McComb JE, Volz RG. Tendon rupture following local steroid injection: report of four cases. Postgrad Med 1980; 68: 169-76.
- Ford LT, DeBender J. Tendon rupture after local steroid injection. South Med J 1979; 72: 827-30.
- Hollander JL. Intrasynovial corticosteroid therapy in arthritis. Md Med J 1970; 19: 62-6.
- Salvarani C, Cantini F, Olivieri I et al. Corticosteroid injections in polymyalgia rheumatica: a double-blind, prospective, randomized, placebo controlled study. J Rheumatol 2000; 27: 1470-6.